For many families, particularly those raising neurodivergent children (e.g., children diagnosed with autism spectrum disorder (ASD), attention-deficit/hyperactivity disorder (ADHD), or other developmental disorders), bedtime can feel overwhelming. What should be a routine often becomes the most challenging adaptive daily living skill of the day. Parents frequently report that getting their child to bed takes hours and is the hardest part of the daily schedule.
Children with ASD often manage a full day that includes school, therapies, meals, and extracurricular activities. By the time bedtime arrives, it can feel like “one more demand.” While parents may view bedtime as a biological necessity, for the child, the instruction “Time for bed” can function as an antecedent for a behavioral event rather than a signal for sleep.
Research has demonstrated that consistent nighttime routines are supported. Predictable bedtime routines improve sleep outcomes, reduce bedtime resistance, and support improved daytime behavior and overall family functioning (Hale et al., 2011; Henderson & Jordan, 2010; Mindell et al., 2009, as cited in Mindell et al., 2017).
Why Do Nighttime Routines Work?
From an Applied Behavior Analysis (ABA) perspective, a bedtime routine consists of a predictable series of signals or cues, known as discriminative stimuli (SDs), that are arranged into a sequence of behaviors called a behavior chain. Each step in this chain leads to a positive outcome, or reinforcement, such as rest, comfort, attention, or relaxation. When families use this routine consistently, it limits the chances for children to engage in avoidance behaviors (escape-maintained) or behaviors seeking attention (attention-maintained) during bedtime. Completing each part of the routine acts as a prompt for beginning the next step in the sequence.
Through consistent routines, children learn:
● A predictable sequence of events, reducing anxiety, avoidance, and negotiation
● Increased engagement in appropriate and replacement behaviors that lead to access to preferred stimuli functioning as reinforcement (e.g., preferred books, calm connection time)
● How to transition from highly stimulating activities to low-stimulation, low-preferred activities
These research findings support the argument that establishing consistent bedtime routines is critical for improving both compliance and overall functioning in families with neurodivergent children. For example, Sytsma et al. (2001, as cited in Larsen & Jordan, 2022) found that predictable environmental cues reinforce compliance and rule-governed behavior, which aligns with the need for structured routines at bedtime. Similarly, Mindell et al. (2009) report that consistent bedtime routines lead to longer sleep duration, and Kitsaras et al. (2018) identify enhancements in child well-being and the parent-child relationship. Subsequently, the effectiveness of a nighttime routine helps to promote positive sleep and behavioral outcomes.
What Does a Consistent Nighttime Routine Consist Of?
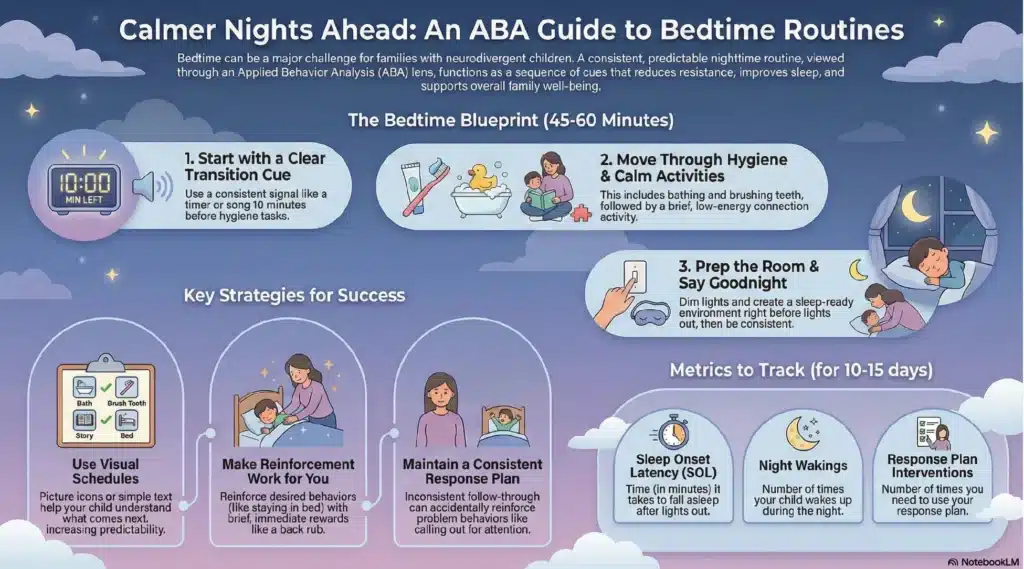
Nighttime routines should be viewed as a structured, teachable process designed to promote regulation and reduce behavioral escalation. Initiating routines approximately 45 to 60 minutes before lights out provides sufficient time for children to gradually transition from stimulating daily activities to restful behaviors, thereby supporting physiological and behavioral readiness for sleep.
Nighttime Routine Sequence
- Transition Cue (~10 minutes before hygiene tasks)
Provide a clear, consistent transition signal to indicate that the routine is beginning. This may include a visual timer, a visual schedule, a consistent verbal cue, or a transition song. Pair the cue with movement toward the bathroom.
Note: Liquids should be discontinued at least 1 hour before/prior to sleep when possible.
Example: The same song nightly paired with the verbal SD, “Bath time.” - Hygiene Chain (15–30 minutes)
This includes bathing or showering, toothbrushing, and changing into pajamas.
Allowing the child to select pajamas either prior to the transition or as part of the routine can increase compliance and reduce resistance. - Connection and Calm (5–10 minutes)
This step should involve a brief, predictable, low-energy activity such as reading, prayer, mindfulness, or a simple puzzle. Activities should promote regulation rather than overstimulation. We want to pair being calm with the start of the sleep process.
During this phase, avoid screentime, as blue light interferes with sleep onset. - Sleep Environment and Final Cue (~2 minutes)
The environment should facilitate sleep. Set up the environment by dimming the lights, adjusting the room temperature, initiating white/pink/brown noise if appropriate, and introducing calming supports (e.g., a weighted blanket when clinically indicated). - Lights Out and Response Plan
Once the lights are out, be consistent in following through on the response plan for calling out or bedtime-delay behaviors.
Bedtime Routines Using ABA Strategies
Visual Schedules
Visual schedules support predictability and task completion.
● Use picture icons or simple text for each step
● Provide praise as each step is completed
● Deliver descriptive praise after completion of the full routine
A First/Then board may be helpful for more challenging steps (e.g., First, brush teeth; then, story).
Make the Reinforcement Do the Work
You will want to avoid extending tablet time, snacks, or play within the routine. Prolonging the nighttime routine can reinforce undesirable behaviors. Instead, try using:
● Use differential reinforcement to reinforce appropriate behaviors (e.g., task completion, remaining in bed, calm behavior)
● Reinforce alternative behaviors that are incompatible with delay or escape
● Provide reinforcement following lights out (e.g., brief back rub, quiet song, or token delivered within 2–3 seconds)
Providing reinforcement should encompass consistent, brief, and clearly contingent on the completion of the routine.
Selecting and Maintaining a Response Plan
There is an increase in persistent problem behavior when follow-through is inconsistent. Behavior is reinforced by contact and may escalate when attention is added. If a child calls out and receives attention after prolonged calling (e.g., 10+ minutes), the behavior is reinforced by contact and may escalate over time.
Response plan options include:
● Graduated check-ins: Brief, scheduled visual checks every 15–30 minutes without verbal interaction
● Planned ignoring: Used for attention-maintained behavior when the child is safe
● Return to bed: Calm redirection without verbal engagement
● Appropriate requesting: Reinforce one appropriate request (vocal or AAC), then signal
● closure (e.g., “All done”)
Collaboration with the child’s BCBA and treatment team is recommended to identify the function of bedtime behavior and ensure ethical and effective implementation.
Difficulty With Sleep Onset
If your child is taking a long time to fall asleep, it may be worth consulting a doctor. If you have tried shifting the bedtime routine later to help the child wake up when they are supposed to get up to start the day, there may be something else at play. We always advise conferring with your child’s primary care physician or medical treatment team when there are issues with their sleep.
Tracking Progress
As a data-driven field, ABA emphasizes objective measurement to support review. Data collection for 10–15 days is recommended:
● Sleep onset latency (SOL): This is the number of minutes it takes for your child to fall asleep after lights out.
● Night wakings: Frequency and duration throughout the night.
● Response plan implementation: The number of required interventions implemented during the night.
Data can be collected using paper tracking or mobile applications and should be reviewed collaboratively with your child’s treatment team. There may be some adjustments needed to improve the routine.
Final Thoughts
Establishing a nighttime routine is not about being strict. However, it’s about maintaining a consistent routine to create a predictable schedule. The routine helps reduce the stress and anxiety often associated with bedtime. Predictability supports regulation and allows the child to anticipate the sequence of steps that comprise the bedtime process (Larsen & Jordan, 2022).
As a family, it is crucial to commit to consistency long enough for a routine pattern to develop. There may be instances when certain steps need to be simplified, but ultimately, following through on the established routine remains important.
Always remember that you can do it!
References
Hale, L., Berger, L. M., LeBourgeois, M. K., & Brooks-Gunn, J. (2011). A longitudinal study of preschoolers’ language-based bedtime routines, sleep duration, and well-being. Journal of Family Psychology, 25(3), 423–433. https://doi.org/10.1037/a0023564
Henderson, J. A., & Jordan, S. S. (2010). Development and preliminary evaluation of the Bedtime Routines Questionnaire. Journal of Psychopathology and Behavioral Assessment, 32(2), 271–280. https://doi.org/10.1007/s10862-009-9143-3
Kitsaras, G., Goodwin, M., Allan, J., Kelly, M. P., & Pretty, I. A. (2018). Bedtime routines and child wellbeing: A systematic review. BMC Public Health, 18(1), Article 386. https://doi.org/10.1186/s12889-018-5290-3
Larsen, K. L., & Jordan, S. S. (2022). Factors associated with consistent bedtime routines and good sleep outcomes. Children’s Health Care, 51(2), 139–162. https://doi.org/10.1080/02739615.2021.1981331
Mindell, J. A., Leichman, E. S., Lee, C., Williamson, A. A., & Walters, R. M. (2017). Implementation of a nightly bedtime routine: How quickly do things improve? Infant Behavior and Development, 49, 220–227. https://doi.org/10.1016/j.infbeh.2017.09.013
Mindell, J. A., Telofski, L. S., Wiegand, B., & Kurtz, E. S. (2009). A nightly bedtime routine: Impact on sleep in young children and maternal mood. Sleep, 32(5), 599–606. https://doi.org/10.1093/sleep/32.5.599
Sytsma, S. E., Kelley, M. L., & Wymer, J. H. (2001). Development and initial validation of the Child Routines Inventory. Journal of Psychopathology and Behavioral Assessment, 23(4), 241–251. https://doi.org/10.1023/A:1012727419873